- Home
- Informazioni di Base
- Feed dalla letteratura
- Prospettive PNEI
- Immunergic Neurotransmission
- Filosofia PNEI
- Sui Passi della Felicità
- Iconografia
- Master PNEI UnivAq (SIPNEI)
- Master Interateneo II Livello
- Link Esterni
- Risorse Bibliografiche
- Annunci pubblicitari
- Dedica
- Chiedi una consulenza
- Sostienici
PsicoNeuroEndocrinoImmunologia
PsicoNeuroEndocrinoImmunologia
Una finestra sul mondo della PNEI
Home » Immunergic Neurotransmission
Immunergic Neurotransmission
Premise
The theory described in this section has been conceived by Dr. Stefano Mancini during his studies on the functioning of antibody response. The term “immunergic neurotransmission” has been coined by Dr. Stefano Mancini, refering to the action of the antibodies as neurotransmitters.
Dr. Mancini wants to thank those who helped him in this work:
Dr. Francesco Mariani
Prof. Luca Roncucci
Dr.ssa Claudia Degli Esposti
Dr. Ronny Cicola.
Have a nice reading!
05-04-2012 commenti (38)
-
Antibodies as Neurotransmitters: A Theory for the Understanding of the Complexity of Neuroimmune Crosstalk and Whole Body Homeostasis.
Introduction
Since the Nobel prize winner Niels K. Jerne suggested the possibility that immune system is regulated by an intricate network of interacting molecules (idiotype network theory, 1976), immune system has not only been interpreted as the self/non-self recognizing apparatus, but also as a gateway by which homeostasis perturbation can result in immune reactivity or immune tolerance[1,2].
Immune system is regulated at many levels by interactions between hormones[3,4], brain peptides[5,6,7], cytokines[8,9], chemokines[10,11], vitamins[12-14], inflammatory mediators[15,16], and a great number of receptors (including Toll-like receptors[17,18] and others[19-22]). The complexity of this tight communication between systems influences different patterns of activation and response of our immune system. The levels of activity of these connections are reciprocal and multidirectional, as it has been documented in many research works since the late 1980s[23-25].
Today, studies addressed in elucidating which antibodies are directed to which antigens and the impact antibodies have in the development of different diseases are exponentially growing, with the implementation of new methods and techniques[26]. This approach is producing a plethora of new antibodies that researchers are trying to characterize in a statistical relationship with different clinical conditions. Anyway, we must admit that for a large part of cases the significance of the presence of circulating antibodies remains poorly understood. In many clinical or experimental situations, antibody production seems inevitably to remain an “epiphenomenon” (i.e. cross-reactivities without a clear role). For an overview of the problematics regarding circulating antibody significance we suggest a selection of the literature[27-39].
Our plasma cells produce a lot of antibodies and if the sense of antibody production were only the interaction with non-self, it would be excessively dispersive for the economy of the individuals and would not be in accordance with the growing evidence of an immune system subjected to genetic and evolutionally selected pattern of antibody reactivity[40-43]. Only in few cases, presence of autoantibodies may predict the development of pathological conditions[29-31] or its course in the years[32,33,36]. On the other side, circulating antibody significance and role are yet showing contrasting evidences[27,34,35,37]. The presence and permanence of myriads of different antibodies following infectious diseases, vaccinations, cancers, pollutant exposures, etc... or even in apparently healthy subjects remains a fascinating conundrum[38,39,44-49]. Finally, the production of antibodies in patients with autoimmune diseases treated with biological therapies (i.e. TNF-alpha blocker monoclonal antibodies, and others) is a paradoxical event that has not yet a clear explanation[50,51].
05-04-2012 commenti (0)
-
Development of the immunergic neurotransmission theory
Evolution has led our body to conjugate efficacy and economy for the simplest coordination between organs and systems. Thus, we could advance the hypothesis that antibodies may operate in a multilevel modality, including the possibility that they may act as neurotransmitters as well as it happens for other molecules in the brain.
In fact, research is clarifying that molecules implicated in the network between nervous, endocrine, and immune systems are redundant. Briefly, a neurotransmitter should be synthesized and stored in nerve terminals, released by a calcium-dependent mechanism, and then inactivated by enzymes in the synaptic cleft and/or by neuronal re-uptake; properties of neurotransmitters have been furnished many years ago by Eccles and other researchers[52-54]. But this approach to neurotransmission is schematic, and does not represent the real complexity of neural interconnections as well as their linkage with hormonal and immune systems. First, it does not take into account the mounting importance of astroglial modulation of neurotransmission, started to be clarified only in the last fifteen years[55-58]. Then, the last twenty years has seen the raise of serotoninergic, histaminergic, purinergic, nitrergic, gamma-aminobutyric acid (GABA)-ergic, cannabinergic, tachykininergic, enkephalinergic, and endorphinergic neurotransmission systems as fundamental typologies of communication in central and peripheral neurons, and receptors for these neurotransmitters are also expressed on lymphocytes and other immune cells[59-67].
Along with these developments in the understanding of the neuro-immune network mediators, interesting are the advancements in the comprehension of the role of the blood-brain barrier (BBB). Though BBB crossing remains a hard challenge for intravenously administered monoclonal antibodies[68], increasing evidences are showing that there may be a passage of natural antibodies through the BBB, or the recruitment of B cells within it, allowing antibodies to interact with the nervous system tissues[69-75].
Basing on these assumptions, we developed an immunergic hypothesis of neurotransmission involving antibody interactions within the nervous system. Experimental results show that B cells, once differentiated in plasma cells, are able to produce antibodies either within or outside the nervous system[72,73,75]. It seems that antibodies may act as direct or indirect neurotransmitters, though the supposition of an indirect immunergic neurotransmission can be supported by a greater amount of evidences.
05-04-2012 commenti (0)
-
Indirect immunergic neurotransmission theory
Since the early 1970s, studies demonstrated that antibodies directed toward synaptosomal antigens exist, are inducible, and may affect permeability to neurotransmitters[76,77]. Anyway, BBB was considered a membrane interposed between humoral immunity and neurons, except for some inflammatory conditions in which breakage of BBB was observed[78]. Recent researches demonstrate that BBB is a dynamic structure interposed between blood torrent and nervous structures, influenced by several factors in physiologic and pathologic conditions[79-84]. Interestingly, variations in BBB permeability have been documented after many kind of stimuli, including antibodies themselves[85-90]. This may suggest that antibodies are implicated in the regulation of neuronal activity.
Moreover, clues for an immunergic indirect neurotransmission could be suggested by considering new insights into the pathogenesis of myasthenia gravis (MG), and some other autoimmune disorders of synaptic transmission[90]. MG is characterized by the presence of autoantibodies directed to nicotinic acetylcholine receptors (nAchR) at the postsynaptic neuromuscular junction, with the effect to interfere with cholinergic activation of muscular contraction (so it is a peripheral disease of the neuromuscular transmission). Initially, these autoantibodies seemed to be specific for neuromuscular junctions, but nowadays reports of multilevel interaction are emerging[91]. In particular, there are growing evidences of cross-reaction between nAchR antibodies and other epitopes localized in the central nervous system. Cross-reactivity between antibodies in MG and neuromyelitis optica (NMO) has been reported[92,93]. In these cases, aquaporin-4 (AQP4) water channel auto-antigen is involved, and frequently symptoms are not limited to optic nerve and spinal cord, but also tend to appear as demyelinating disorders of the central nervous system. This cross-reactivity is interesting for the fact that it links peripheral with central nervous system, with passage of autoantibodies inside the brain[92].
These autoantibodies, likewise others seen in several conditions[89,90,94,95], are particularly able to interfere with neuronal transmission and signal homeostasis within the brain, also acting through glial cells and interfering with different excitatory or inhibitory pathways; again, they are associated with enhancing of BBB permeability[87,88,90,96]. These evidences led us to think that a feedback control between immune and nervous system mediated by antibodies could exist. A feedback in which antibodies, along with cytokines and hormones, could play a role in neurotransmission modulation between the “periphery” and the “centre”.
If we take into account that a basal natural autoimmunity is present in healthy people[27], we may suppose that antibody interactions with neurotransmission could be a homeostatic factor for individuals. In other words, antibodies may act as signalling molecules able to connect immune and nervous systems through the modulation of neurotransmission, interacting with different nervous structures. The disruption of this homeostasis may be provoked by the action of particular pathogens in specific neuroendocrine situations, and/or by profound antigenic stimulation due to neoplastic diseases. This could also explain in part a major incidence of immune dysregulation in women, due to higher levels in estrogens which have been associated to different pattern of neurotransmission with respect to men[97,98].
05-04-2012 commenti (0)
-
Direct immunergic neurotransmission theory
Since antibody synthesis is probably one of the most versatile activity of our organism, able to connect our body with the external environment and protect us by any harmful stimuli, we hypothesized that antibodies could also act as mediators between “periphery” and “centre” as direct immunergic neurotransmitters. Obviously, it is difficult to think they could be classical neurotransmitters, since vesicles of antibodies at the synaptic knob have never been observed. However, as it happens for other substances implicated in non-adrenergic-non-cholinergic neurotransmission[5,7,57], we have supposed that they may directly interact with synaptic membrane receptors in order to evocate or inhibit neuronal action potentials.
The direct immunergic hypothesis differs from the indirect one because in the latter antibodies are responsible only for their interference with the action of a “classic” neurotransmitter. In the direct immunergic hypothesis of neurotransmission, antibodies are directly responsible for the releasing of a neurotransmitter (with excitatory or inhibitory function), or they are directly able to evoke a postsynaptic potential by their binding to a neuronal receptor.
In support of this theory, we considered that in patients with systemic lupus erythematosus (SLE) part of the autoantibodies that target dsDNA are able to cross-react with different subunits of the NMDA receptor (NMDAR)[89] producing a spectrum of symptoms comprising cognitive impairment, emotional imbalance, anxiety and, in some cases, seizures and psychosis[99]. It has been shown that anti-NMDAR binding may function as modulator when neuron has activated synapse, probably by increasing the channel open-state duration regulated by glutamate. Different effects have also been documented in relation to antibody titers. Lower or discontinuous titers seemed to produce only electrophysiological changes in NMDAR-mediated synaptic transmission, while higher titers induced neuronal stress and neurotoxicity[89]. Antibodies that target NMDAR are also responsible for the most common type of autoimmune encephalitis, in which they are generally at high titers[100-102] and in patients with no history of SLE. Antibodies targeting CNS receptors and involved in neurotransmission alterations have been documented in several works[45,90,100,101].
Growing evidences that link presence of autoimmunity and psychic status could be an interesting support to our hypothesis that a direct immunergic modulation of neurotransmission is present in healthy individuals. Autoantibodies in low titers are present also in physiologic conditions like many other cytokines and mediators of inflammation. The presence of autoimmune phenomena in psychiatric patients is documented, and on the other side patients with autoimmune diseases frequently have psychiatric symptoms as comorbidities[103-108]. Psychiatric disorders are linked to an augmented inflammatory status, giving support to a tight connection between nervous and immune systems[109-111]. In addition to anti-NMDAR, other antibodies that bind voltage-gate potassium channels have been found in association with psychosis in patients with autoimmune encephalitis[112].
The challenging issue that needs to be clarified is if a different spectrum of disease (or the border between physiologic and pathologic conditions) is related to antibody titers rather than different kinds of circulating antibodies. According to our theory, we think that quantitative rather than qualitative characteristic in antibody production could make the difference between physiologic and pathologic conditions because a basal interaction between neurons and antibodies may be as necessary as basal interaction between other molecules (e.g. cytokines, opioids, brain peptides, etc…) and the nervous system[113,114].
05-04-2012 commenti (0)
-
Concluding remarks
It has been documented by many researches how body homeostasis is the result of the close, continuous, and multidirectional dialogue between nervous, endocrine, and immune systems. In the last decade, enormous progresses have been made into the clarification of the neuroimmune crosstalk, with particular emphasis on the role of neurotransmitters, brain peptides and hormones, due to their ability to spread to, and be shared by, tissues and cells involved in the neuroimmune modulation[3-7,11,22,113-120].
Since recent studies are showing that BBB is a dynamic structure and could also be crossed by antibodies[69-71,90], or there could be an intrathecal synthesis of immunoglobulins[72-75], we hypothesized that the pool of molecules involved in neuroimmune crosstalk could be expanded by the comprehension of antibodies into a circuitry that we have called immunergic neurotransmission, summarized in Figure 1. Our hypothesis is based on the evidence that many pathologic conditions are characterized by an increased synthesis of antibodies for which cross-reactivity between the “periphery” and the “centre” is very frequent. Moreover, significance of the presence of these antibodies is uncertain in many conditions, sometimes affects healthy individuals, and thus is still object of debate[89-95,103].
In conclusion, we hope that our theory, that obviously needs effective experimental proofs, may be a contribution to the development of a new research approach in which antibody production is not a simple response to non-self, but a complex effect of human evolution towards a system fully integrated in the neuroimmune dialogue.
05-04-2012 commenti (0)
-
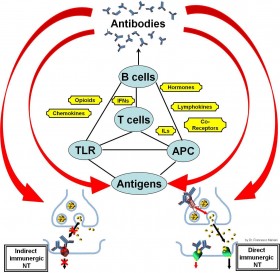
Figure 1.
A schematic overview of the factors involved in neuroimmune crosstalk is illustrated. Antibodies are at the top of the pyramid that represents neuroimmune activation and regulation. Cytokines, brain peptides, hormones, and the other inflammation mediators have a pivotal role in regulating integrated processes between environment (antigens), nervous tissues, and immune cells that ultimately lead to antibody production. In our immunergic neurotransmission hypothesis, antibodies could be in turn the effectors that close in a certain manner the neuroimmune circuit.
Abbreviations: APC: antigen presenting cells, IFNs: interferons, ILs: interleukins, NT: neurotransmission, TLR: Toll-like receptors.
05-04-2012 commenti (0)
-
References
- Shoenfeld Y. The idiotypic network in autoimmunity: antibodies that bind antibodies that bind antibodies. Nat Med 2004;10(1):17-8.
- Jerne NK. Towards a network theory of the immune system. Ann Immunol 1974;
- Grossman CJ. Regulation of the immune system by sex steroids. Endocr Rev 1984;5(3):435-55.
- Paavonen T. Hormonal regulation of lymphocyte functions. Med Biol 1987;65(5-6):229-40.
- Snyder SH. Brain peptides as neurotransmitters. Science 1980;209(4460):976-83.
- O'Dorisio MS. Neuropeptides and gastrointestinal immunity. Am J Med 1986;81(6B):74-82.
- Cavagnaro J,
- Dinarello CA. Interleukin-1. Ann N Y Acad Sci 1988;546:122-32.
- Arai KI, Lee F, Miyajima A, Miyatake S, Arai N, Yokota T. Cytokines: coordinators of immune and inflammatory responses. Annu Rev Biochem 1990;59:783-836.
- Alm GV. Lymphokines in the regulation of immune responses. Vet Immunol Immunopathol 1987;17(1-4):173-82.
- Christopherson K, Hromas R. Chemokine regulation of normal and pathologic immune responses. Stem Cells 2001;19(5):388-96.
- Leibovitz B,
- Manolagas SC, Provvedini DM, Tsoukas CD. Interactions of 1,25-dihydroxyvitamin D3 and the immune system. Mol Cell Endocrinol 1985;43(2-3):113-22.
- Peelen E, Knippenberg S, Muris AH, Thewissen M, Smolders J, Tervaert JW, Hupperts R, Damoiseaux J. Effects of vitamin D on the peripheral adaptive immune system: a review. Autoimmun Rev 2011;10(12):733-43.
- Lewis RA. Interactions of eicosanoids and cytokines in immune regulation. Adv Prostaglandin Thromboxane Leukot Res 1990;20:170-8.
- Kalinski P. Regulation of immune responses by prostaglandin E2. J Immunol. 2012;188(1):21-8.
- Kirschning CJ, Bauer S. Toll-like receptors: cellular signal transducers for exogenous molecular patterns causing immune responses. Int J Med Microbiol 2001;291(4):251-60.
- Bourke E, Bosisio D, Golay J, Polentarutti N, Mantovani A. The toll-like receptor repertoire of human B lymphocytes: inducible and selective expression of TLR9 and TLR10 in normal and transformed cells. Blood 2003;102(3):956-63.
- Nelson RP Jr, Ballow M. Immunomodulation and immunotherapy: drugs, cytokines, cytokine receptors, and antibodies. J Allergy Clin Immunol 2003;111(2 Suppl):S720-43.
- Refojo D, Liberman AC, Giacomini D, Carbia Nagashima A, Graciarena M, Echenique C, Paez Pereda M, Stalla G, Holsboer F, Arzt E. Integrating systemic information at the molecular level: cross-talk between steroid receptors and cytokine signaling on different target cells. Ann N Y Acad Sci 2003;992:196-204.
- Alcami A. Viral mimicry of cytokines, chemokines and their receptors. Nat Rev Immunol 2003;3(1):36-50.
- McCarthy L, Wetzel M, Sliker JK, Eisenstein TK,
- Cavagnaro J. Molecular basis for the bidirectional modulation of the neuroendocrine and the immune systems. Year Immunol 1986;2:303-22.
- Kordon C, Bihoreau C. Integrated communication between the nervous, endocrine and immune systems. Horm Res 1989;31(1-2):100-4.
- Hall NR, O'Grady MP. Regulation of pituitary peptides by the immune system. Bioessays 1989;11(5):141-4.
- Tozzoli R. The diagnostic role of autoantibodies in the prediction of organ-specific autoimmune diseases. Clin Chem Lab Med 2008;46(5):577-87.
- Lleo A, Invernizzi P, Gao B, Podda M, Gershwin ME. Definition of human autoimmunity--autoantibodies versus autoimmune disease. Autoimmun Rev 2010;9(5):A259-66.
- Li QZ, Karp DR, Quan J, Branch VK, Zhou J, Lian Y, Chong BF, Wakeland EK, Olsen NJ. Risk factors for ANA positivity in healthy persons. Arthritis Res Ther 2011;13(2):R38.
- Scofield RH. Autoantibodies as predictors of disease. Lancet 2004;363(9420):1544-6.
- Kokkonen H, Mullazehi M, Berglin E, et al. Antibodies of IgG, IgA and IgM isotypes against cyclic citrullinated peptide precede the development of rheumatoid arthritis. Arthritis Res Ther 2011;13(1):R13.
- Shoenfeld Y, Blank M, Abu-Shakra M, et al. The mosaic of autoimmunity: prediction, autoantibodies, and therapy in autoimmune diseases. 2008 IMAJ;10:13–19.
- Bogdanos DP, Mieli-Vergani G, Vergani D. Autoantibodies and their antigens in autoimmune hepatitis. Semin Liver Dis 2009;29(3):241-53.
- Alaedini A, Green PH. Autoantibodies in celiac disease. Autoimmunity 2008;41(1):19-26.
- Fritzler MJ, Salazar M. Diversity and origin of rheumatologic autoantibodies. Clin Microbiol Rev 1991;4(3):256-69.
- da Mota LM, Dos Santos Neto LL, de Carvalho JF, Pereira IA, Burlingame R, Ménard HA, Laurindo IM. The presence of anti-citrullinated protein antibodies (ACPA) and rheumatoid factor on patients with rheumatoid arthritis (RA) does not interfere with the chance of clinical remission in a follow-up of 3 years. Rheumatol Int 2011 Dec 21;DOI: 10.1007/s00296-011-2260-9.
- Miller A, Chan M, Wiik A, Misbah SA, Luqmani RA. An approach to the diagnosis and management of systemic vasculitis. Clin Exp Immunol 2010;160(2):143-60.
- Borg AA. Antibodies to cytokeratins in inflammatory arthropathies. Semin Arthritis Rheum 1997;27(3):186-95.
- Brás A, Aguas AP. Mycobacteria-induced autoantibody production is associated with susceptibility to infection but not with host propensity to develop autoimmune disease. Clin Exp Immunol 1995;100(1):75-80.
- Ferrara F, Quaglia S, Caputo I, et al. Anti-transglutaminase antibodies in non-coeliac children suffering from infectious diseases. Clin Exp Immunol 2010;159(2):217-23.
- Hodgkin PD An antigen valence theory to explain the evolution and organization of the humoral immune response. Immunol Cell Biol 1997;75(6):604-18.
- Scott-Browne JP, Crawford F, Young MH, Kappler JW, Marrack P, Gapin L. Evolutionarily conserved features contribute to αβ T cell receptor specificity. Immunity 2011;35(4):526-35.
- O'Connell MJ, McInerney JO. Gamma chain receptor interleukins: evidence for positive selection driving the evolution of cell-to-cell communicators in the mammalian immune system. J Mol Evol 2005;61(5):608-19.
- Kasahara M, Suzuki T, Pasquier LD. On the origins of the adaptive immune system: novel insights from invertebrates and cold-blooded vertebrates. Trends Immunol. 2004;25(2):105-11.
- Kanakoudi-Tsakalidou F, Tzimouli V, Pratsidou-Gertsi P, Chronopoulou E, Trachana M. The significance of persistent newly developed autoantibodies in JIA patients under long-term anti-TNF treatment. Cytokine 2008;42(3):293-7.
- Posner JB. Immunology of paraneoplastic syndromes: overview. Ann N Y Acad Sci 2003;998:178-86.
- Thomas C, Moridani M. Interindividual variations in the efficacy and toxicity of vaccines. Toxicology 2010;278(2):204-10.
- de Bruyn G. Cofactors that may influence vaccine responses. Curr Opin HIV AIDS 2010;5(5):404-8.
- Thrasher JD, Broughton A, Madison R. Immune activation and autoantibodies in humans with long-term inhalation exposure to formaldehyde. Arch Environ Health 1990;45(4):217-23.
- El-Fawal HA, Waterman SJ, De Feo A, Shamy MY. Neuroimmunotoxicology: humoral assessment of neurotoxicity and autoimmune mechanisms. Environ Health Perspect 1999 Oct;107 Suppl 5:767-75.
- Tracey D, Klareskog L, Sasso EH, Salfeld JG, Tak PP. Tumor necrosis factor antagonist mechanisms of action: a comprehensive review. Pharmacol Ther 2008;117:244–279.
- Mancini S, Amorotti E, Vecchio S, Ponz de Leon M, Roncucci L. Infliximab-related hepatitis: discussion of a case and review of the literature. Intern Emerg Med 2010 Jun;5(3):193-200.
- Eccles JC. Excitatory and inhibitory synaptic action. Ann N Y Acad Sci 1959;81:247-64.
- von Euler
- Schloesser R, Simkowitz P, Bartlett EJ, Wolkin A, Smith GS, Dewey SL, Brodie JD. The study of neurotransmitter interactions using positron emission tomography and functional coupling. Clin Neuropharmacol 1996;19(5):371-89.
- Eroglu C, Barres BA. Regulation of synaptic connectivity by glia. Nature 2010;468(7321):223-31.
- Perea G, Araque A. GLIA modulates synaptic transmission. Brain Res Rev 2010;63(1-2):93-102.
- Pannasch U, Vargová L, Reingruber J, et al. Astroglial networks scale synaptic activity and plasticity. Proc Natl Acad Sci U S A 2011;108(20):8467-72.
- López-Muñoz F, Alamo C. Historical evolution of the neurotransmission concept. J Neural Transm 2009;116(5):515-33.
- Llewellyn-Smith IJ. Anatomy of synaptic circuits controlling the activity of sympathetic preganglionic neurons. J Chem Neuroanat 2009;38(3):231-9.
- Mulè F, Amato A, Baldassano S, Serio R. Evidence for a modulatory role of cannabinoids on the excitatory NANC neurotransmission in mouse colon. Pharmacol Res 2007;56(2):132-9.
- El-Mahmoudy A, Matsuyama H, Khalifa M, Shimizu Y, Takewaki T. Tachykinins mediate non-adrenergic, non-cholinergic excitatory neurotransmission to the hamster ileum via NK1 and NK2 receptors. Life Sci 2003;73(15):1939-51.
- Elde R, Arvidsson U, Riedl M, et al. Distribution of neuropeptide receptors. New views of peptidergic neurotransmission made possible by antibodies to opioid receptors. Ann N Y Acad Sci 1995;757:390-404.
- van der Stelt M, Di Marzo V. The endocannabinoid system in the basal ganglia and in the mesolimbic reward system: implications for neurological and psychiatric disorders. Eur J Pharmacol 2003;480(1-3):133-50.
- Rand MJ. Nitrergic transmission: nitric oxide as a mediator of non-adrenergic, non-cholinergic neuro-effector transmission. Clin Exp Pharmacol Physiol 1992;19(3):147-69.
- Bustamante S, Orensanz LM, Recio P, Carballido J, García-Sacristán A, Prieto D, Hernández M. Functional evidence of nitrergic neurotransmission in the human urinary bladder neck. Neurosci Lett 2010;477(2):91-4.
- Zhang Z, Bhalla A, Dean C, Chapman ER, Jackson MB. Synaptotagmin IV: a multifunctional regulator of peptidergic nerve terminals. Nat Neurosci 2009;12(2):163-71.
- Frank RT,
- Drlicek M, Liszka U, Jellinger K, Mohn-Staudner A, Lintner F, Grisold W. Circulating antineuronal antibodies reach neurons in vivo: an autopsy study. J Neurol 1992;239(7):407-10.
- Sas A, Jones R, Tyor W. Intra-peritoneal injection of polyclonal anti-interferon alpha antibodies cross the blood brain barrier and neutralize interferon alpha. Neurochem Res 2008;33(11):2281-7.
- Levin EC, Acharya NK, Han M, Zavareh SB, Sedeyn JC, Venkataraman V, Nagele RG. Brain-reactive autoantibodies are nearly ubiquitous in human sera and may be linked to pathology in the context of blood-brain barrier breakdown. Brain Res 2010;1345:221-32.
- Xiao BG, Link H. Immune regulation within the central nervous system. J Neurol Sci 1998 Apr 15;157(1):1-12.
- Ransohoff RM, Cardona AE. The myeloid cells of the central nervous system parenchyma. Nature 2010;468(7321):253-62.
- Man S, Tucky B, Cotleur A, Drazba J, Takeshita Y,
- Knopf PM, Harling-Berg CJ, Cserr HF, et al. Antigen-dependent intrathecal antibody synthesis in the normal rat brain: tissue entry and local retention of antigen-specific B cells. J Immunol 1998;161(2):692-701.
- Raiteri M, Bertollini A,
- Raiteri M, Levi G. Antisynaptosome antibodies affect synaptosomal permeability to neurotransmitters. Nat New Biol 1973;245(142):89-91.
- Ribatti D, Nico B, Crivellato E, Artico M. Development of the blood-brain barrier: a historical point of view. Anat Rec B New Anat 2006;289(1):3-8.
- Ohtsuki S. New aspects of the blood-brain barrier transporters; its physiological roles in the central nervous system. Biol Pharm Bull 2004;27(10):1489-96.
- Johansson PA, Dziegielewska KM, Liddelow SA, Saunders NR. The blood-CSF barrier explained: when development is not immaturity. Bioessays 2008;30(3):237-48.
- Banks WA. The blood-brain barrier in psychoneuroimmunology. Neurol Clin 2006;24(3):413-9.
- Banks WA. Blood-brain barrier as a regulatory interface. Forum Nutr 2010;63:102-10.
- Abbott NJ, Patabendige AA, Dolman DE, Yusof SR, Begley DJ. Structure and function of the blood-brain barrier. Neurobiol Dis 2010;37(1):13-25.
- Engelhardt B, Sorokin L. The blood-brain and the blood-cerebrospinal fluid barriers: function and dysfunction. Semin Immunopathol 2009;31(4):497-511.
- Dankbaar JW, Hom J, Schneider T, Cheng SC, Lau BC, van der Schaaf I, Virmani S, Pohlman S, Wintermark M. Age- and anatomy-related values of blood-brain barrier permeability measured by perfusion-CT in non-stroke patients. J Neuroradiol 2009;36(4):219-27.
- Larochelle C, Alvarez JI, Prat A. How do immune cells overcome the blood-brain barrier in multiple sclerosis? FEBS Lett 2011;585(23):3770-80.
- Vincent T, Saikali P, Cayrol R, Roth AD, Bar-Or A, Prat A, Antel JP. Functional consequences of neuromyelitis optica-IgG astrocyte interactions on blood-brain barrier permeability and granulocyte recruitment. J Immunol 2008;181(8):5730-7.
- Kanda T, Yamawaki M, Iwasaki T, Mizusawa H. Glycosphingolipid antibodies and blood-nerve barrier in autoimmune demyelinative neuropathy. Neurology 2000;54(7):1459-64.
- Faust TW, Chang EH, Kowal C, et al. Neurotoxic lupus autoantibodies alter brain function through two distinct mechanisms. Proc Natl Acad Sci U S A 2010;107(43):18569-74.
- Whitney KD, McNamara JO. Autoimmunity and neurological disease: antibody modulation of synaptic transmission. Annu Rev Neurosci 1999;22:175-95.
- Vaknin-Dembinsky A, Abramsky O, Petrou P, et al. Myasthenia gravis-associated neuromyelitis optica-like disease: an immunological link between the central nervous system and muscle? Arch Neurol 2011 Dec;68(12):1557-61.
- Miyazaki Y, Hirayama M, Watanabe H, Usami N, Yokoi K, Watanabe O, Sobue G. Paraneoplastic encephalitis associated with myasthenia gravis and malignant thymoma. J Clin Neurosci 2012 Feb;19(2):336-8.
- Wang Z, Low PA, Jordan J, et al. Autoimmune autonomic ganglionopathy: IgG effects on ganglionic acetylcholine receptor current. Neurology 2007;68(22):1917-21.
- Vernino S. Neuronal acetylcholine receptor autoimmunity. Ann N Y Acad Sci 2008;1132:124-8.
- Hinson SR, McKeon A, Lennon VA. Neurological autoimmunity targeting aquaporin-4. Neuroscience 2010;168(4):1009-18.
- Sárvári M, Kalló I, Hrabovszky E, et al. Estradiol replacement alters expression of genes related to neurotransmission and immune surveillance in the frontal cortex of middle-aged, ovariectomized rats. Endocrinology 2010;151(8):3847-62.
- Czlonkowska A, Ciesielska A, Gromadzka G, Kurkowska-Jastrzebska I. Estrogen and cytokines production - the possible cause of gender differences in neurological diseases. Curr Pharm Des 2005;11(8):1017-30.
- Appenzeller S, Costallat LT, Cendes F. Neurolupus. Arch Neurol 2006;63(3):458-60.
- Irani SR, Vincent A. Autoimmune encephalitis -- new awareness, challenging questions. Discov Med 2011;11(60):449-58.
- Graus F, Dalmau J. CNS autoimmunity: new findings and pending issues. Lancet Neurol 2012;11(1):17-9.
- Barry H, Hardiman O, Healy DG, et al. Anti-NMDA receptor encephalitis: an important differential diagnosis in psychosis. Br J Psychiatry 2011;199(6):508-9.
- Kayser MS, Dalmau J. The emerging link between autoimmune disorders and neuropsychiatric disease. J Neuropsychiatry Clin Neurosci 2011;23(1):90-7.
- Tanaka S, Matsunaga H, Kimura M, et al. Autoantibodies against four kinds of neurotransmitter receptors in psychiatric disorders. J Neuroimmunol 2003;141(1-2):155-64.
- Benros ME, Nielsen PR, Nordentoft M, Eaton WW, Dalton SO, Mortensen PB. Autoimmune diseases and severe infections as risk factors for schizophrenia: a 30-year population-based register study. Am J Psychiatry 2011;168(12):1303-10.
- Zandi MS, Irani SR, Lang B, et al. Disease-relevant autoantibodies in first episode schizophrenia. J Neurol 2011;258(4):686-8.
- Kayser MS, Kohler CG, Dalmau J. Psychiatric manifestations of paraneoplastic disorders. Am J Psychiatry 2010;167(9):1039-50.
- Padmos RC, Bekris L, Knijff EM, et al. A high prevalence of organ-specific autoimmunity in patients with bipolar disorder. Biol Psychiatry 2004;56(7):476-82.
- Raedler TJ. Inflammatory mechanisms in major depressive disorder. Curr Opin Psychiatry 2011;24(6):519-25.
- Dean B. Understanding the role of inflammatory-related pathways in the pathophysiology and treatment of psychiatric disorders: evidence from human peripheral studies and CNS studies. Int J Neuropsychopharmacol 2011;14(7):997-1012.
- Pizzi C, Manzoli L, Mancini S, Costa GM. Analysis of potential predictors of depression among coronary heart disease risk factors including heart rate variability, markers of inflammation, and endothelial function. Eur Heart J 2008 May;29(9):1110-7.
- Ganguli A, Fitzgerald R, Walker L, Beadsworth M, Mwandumba HC. Voltage-gated, potassium-channel antibody-associated limbic encephalitis presenting as acute psychosis. J Neuropsychiatry Clin Neurosci 2011;23(2):E32-4.
- Haddad JJ,
- Haddad JJ. On the mechanisms and putative pathways involving neuroimmune interactions. Biochem Biophys Res Commun 2008;370(4):531-5.
- Huang D, Han Y, Rani MR, et al. Chemokines and chemokine receptors in inflammation of the nervous system: manifold roles and exquisite regulation. Immunol Rev. 2000;177:52-67.
- Kin NW, Sanders VM. It takes nerve to tell T and B cells what to do. J Leukoc Biol 2006;79(6):1093-104.
- Fischer EG. Opioid peptides modulate immune functions. A review. Immunopharmacol Immunotoxicol 1988;10(3):265-326.
- Matsuda T, Yamasaki K, Taga T, Hirano T, Kishimoto T. Current concepts of B cell modulation. Int Rev Immunol 1989;5(2):97-109.
- Madden KS, Sanders VM, Felten DL. Catecholamine influences and sympathetic neural modulation of immune responsiveness. Annu Rev Pharmacol Toxicol 1995;35:417-48.
- Qiu Y, Peng Y, Wang J. Immunoregulatory role of neurotransmitters. Adv Neuroimmunol 1996;6(3):223-31.
05-04-2012 commenti (0)
TESTI DI RIFERIMENTO

Psychoneuroimmunology by Ader

Testo di ampio respiro PNEI, curato da LA Wisneski e L Anderson.
Psychoneuroimmunology by Schedlowski and Tewes
Psychoneuroimmunology by Goodkin and Visser

Psychoneuroendocrinology by Wolkowitz and Rothschild

Psychoneuroendocrinology by Czerbska
Psychoneuroimmunology: hypothesis and current research, by Sperner-Unterweger, Fleischhacker, Kaschka.

Psychoneuroimmunology: a behavioral approach. By Singh, Shyam and Singh.
Fundamentals of Psychoneuroimmunology by Song and Leonard

Stress Science: Neuroendocrinology by Fink

Study guide to Psychosomatic Medicine by Bourgeois, Hales and Shahrokh

Human Psychoneuroimmunology by Kavita Vedhara and Michael Irwin

The link between Religion and Health - Psychoneuroimmunology and the Faith Factor by HG Koenig and HJ Cohen
Mind-Body Medicine by Alan Watkins
The Handbook of Stress Science by R.J. Contrada and A. Baum

Stress Management by W. Linden

Handbook of Neuroendocrinology, First Ed, 2012, by Fink G., Pfaff D., Levine J.
Nuova edizione del classico curato da HG Koenig.
Seconda edizione del testo curato da JH Daruna.

Recente testo curato da SC Segerstrom.

The Wiley Blackwell Handbook of Psychoneuroimmunology, curato da AW Kusnecov e H Anisman.
Testo base curato da J.E. Blalock, pioniere della PNEI.
Autore R.C. Gaillard, forte impostazione sperimentale.

Sistema immunitario e tessuto nervoso: dalla fisiologia alla patologia.

Stahl's Essential Psychopharmacology: Neuroscientific Basis and Practical Applications di Stephen M. Stahl, 2013
The American Psychiatric Publishing Textbook of Psychopharmacology a cura di Alan F. Schatzberg, Charles B. Nemeroff